 Headache is a common presenting complaint for patients in ED, and it is important to be able to differentiate between a 'primary headaches' and 'secondary headaches'. Primary headaches are the 'BIG THREE' and are not caused by an underlying medical condition: - Migraine -Tension type headache - Cluster headache Secondary headaches - Are due to an underlying condition and can be much more serious. Most headaches you'll see in ED will be in the first category of a 'primary headache' and of these, the majority will be migraines. In this lunchtime learning session we'll focus on how to diagnose and treat migraine, and also cover some 'red flags' to look out for which should make you think about the possibility of a 'secondary' cause of headache. HOW TO DIAGNOSE MIGRAINE? HISTORY: Migraine is a clinical diagnosis - meaning that it's a diagnosis made by history and examination. Always ask about RED FLAGS in a headache history (covered at the end of this teach). Consider a gross neurological examination in patients presenting with headache. A useful mnemonic to remember the key features of migraine is POUND Think if I had a 'pound' for everytime I saw a patient with a migraine I'd be rich! 
The more of these criteria your patient has the more likely it is to be migraine. Patients with 4 or more of these symptoms have a likelyhood ratio of 24 or a sensitivity of 92% in primary care. Other symptoms that may be present:
Same old symptoms? Or NEW?: Its important to establish if the patient previously suffers from headaches or has a known diagnosis of migraine. If they do, it's important to establish if the symptoms they are having are the same or different to their normal headaches. If the symptoms are new or different this should raise the possibility of an alternative diagnosis and prompt you to consider senior review of the patient/further investigations. TREATMENT OF MIGRAINE: Environment:
Analgesia: Remember the pain ladder:
Antiemetics:
Specific drugs for migraine:
To admit or not?:
WHAt DO WE MEAN BY RED FLAGS? Red flags are symptoms that you should ask about in your headache history that raise the possibility of a secondary cause of headache. If these are present consider a senior review of the patient +/- further investigations/admission. RED FLAGS:
What conditions can these red flags be signs/symptoms of? The diagram below is not a comprehensive list but gives you an idea of other things to consider if red flags are present: 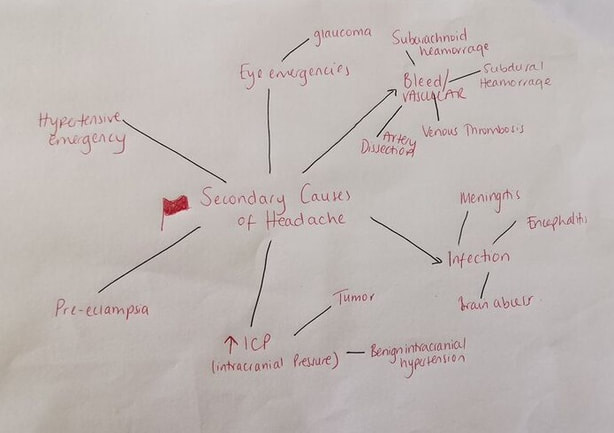 References:
Dr Alice Hunter
0 Comments
We have recently updated the departmental chest pain pathway. When a patient presents with chest pain suspicious for cardiac ischaemia an ECG should be performed immediately. Not all patients with critical ischaemia present with ST-Elevation on their ECG. The ECG patterns below are STEMI equivalents and if found in a patient with the right clinical presentation should prompt an urgent senior review with early discussion with cardiology. 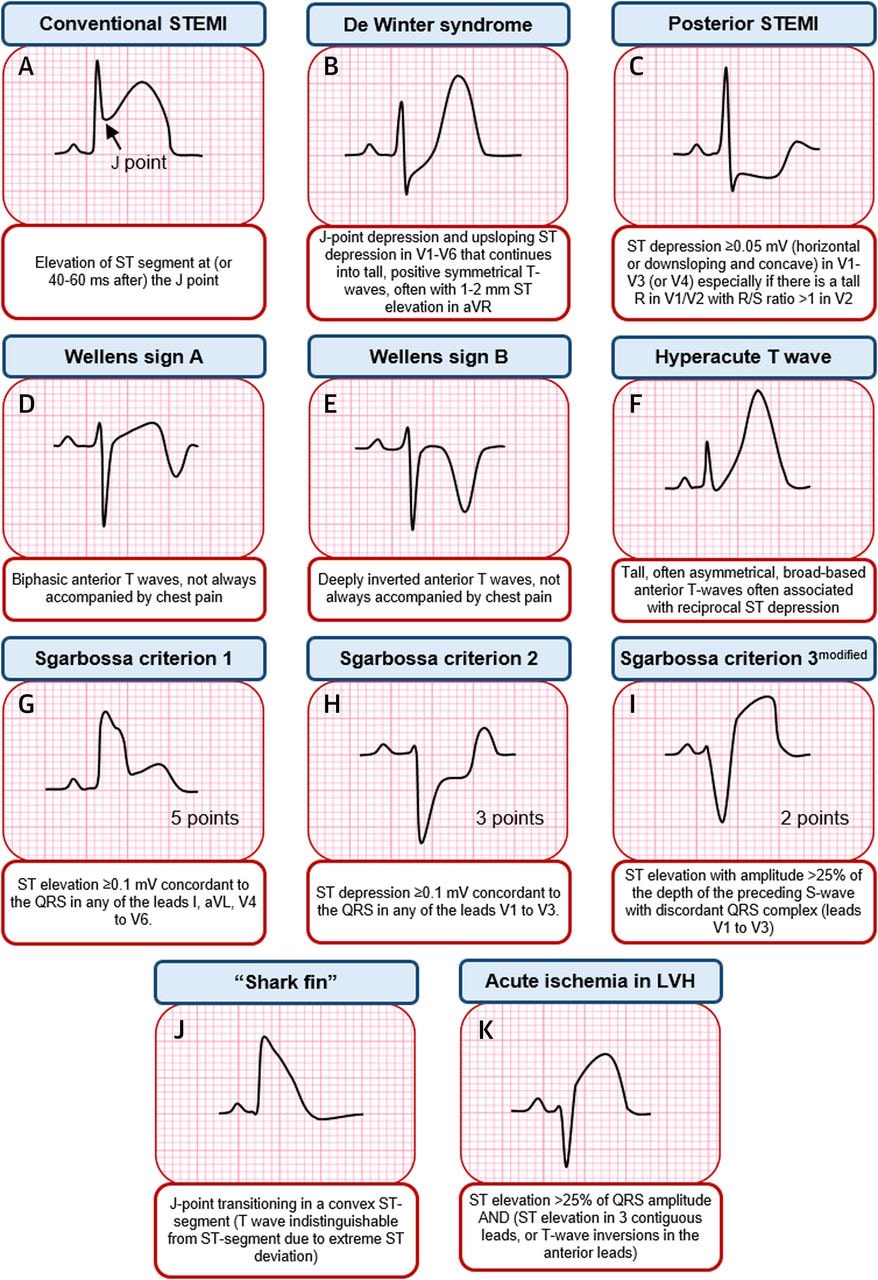 Source: Asatryan B et al,Electrocardiographic diagnosis of life threatening STEMI Equivalents, JACC:case reports, 2019, 1(4)
Dr Martin Dore Tetanus is an infection caused by the anaerobic bacteria clostridium tetani which is found in soil and manure. Tetanus infection has a 90% mortality, but thankfully due to the success of vaccinations, it is rare with only 4 cases in the UK in 2019. Patients often rock up to ED because someone told them they “might need a tetanus” and the guidelines have recently changed as to who needs a booster/immunoglobulin, so hopefully this little 5 step plan should demystify it for you! STEP 1: ASSESS THE WOUND:
Tetanus-prone:
Tetanus high risk wound: is any of the above PLUS
Clean:
Note - A wound can't be tetanus high risk unless its already tetanus prone Remember that ALL wounds require thorough washout with clean water or normal saline. STEP 2: WHATS THE PATIENTS IMMUNISATION STATUS? So now you know what category the patients wound is in, the next question is whats the patient's immunisation status! Remember a full Course of tetanus vaccinations is 5 doses. A ‘priming course’ means 3 doses which is given in childhood. The table below is from the ‘green book’ on tetanus, simplified below: 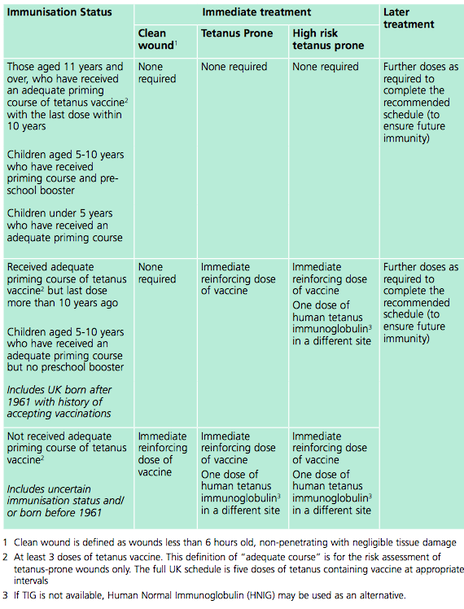 IN SIMPLER TERMS:
The main change in the guidance is that any adult who hasn't had a booster for 10 years with a tetanus prone wound now needs a booster! It used to be that if you'd had your full childhood immunisations then this wasn't indicated, so make sure your patient knows when their last booster was! STEP 3: WHAT DOSE DO I PRESCRIBE?: Tetanus Booster: Revaxis is the name of the tetanus booster and is a 3 in 1 diphtheria, tetanus + polio vaccine. Give one 0.5ml syringe. Immunoglobulin: For most cases 250 iu by IM injection If >24 hours have elapsed since the injury, or there is a risk of heavy contamination or burns then 500iu by IM injection. STEP 4: WHERE DO I FIND IT IN ED?: Tetanus booster- This is called ‘Revaxis’ and lives in the drugs fridge in resus. Attach a green needle directly to the syringe and its ready to be given IM! There’s a small sticker with a barcode on the side of the syringe which you should stick on the ED card next to where you sign for giving the drug. Tetanus immunoglobulin – This is technically a ‘blood product’ in the trust. Which means that you need to call blood bank and inform them that your patient needs immunoglobulin and have their details handy and the dose you require. When the tetanus is ready it will be available for the nurses to see on ‘blood track’ and they need to print a pick up slip to take to pick it up. This usually takes about 20-30 minutes. Doctors cannot pick this up, but can give the injection if you have a barcode for the blood transfusion machine. When you have the immunoglobulin you need to print the patient a wrist band and take the blood transfusion scanning machine with you to the patient – doing an ID check and scanning the square barcode on the side of the immunoglobulin (if you do not do this the lab will call up and will ask you to!) What if I need to give a booster AND Immunoglobulin? – inject IM in two different sites- i.e.:one arm each. STEP 5: ONGOING CARE:
References: The very long full government guidelines on tetanus immunisations: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/859519/Greenbook_chapter_30_Tetanus_January_2020.pdf Dr Alice Hunter |
This will be an archive of learning blogs and lunchtime learnings bites!
Archives
February 2023
Categories
All
|
 RSS Feed
RSS Feed