|
Winter has finally arrived and a new season brings new environmental factors that may play a part in a patients presentation. As we move into the coldest months of the year the identification and management of hypothermia is something which we may all need to revise. Hypothermia can be categorised into: Mild - 32-35'C Moderate- 28 - 32'C Severe - less than 28'C In these cold months be sure to consider hypothermia in elderly patients and the young when presenting acutely unwell. The identification of hypothermia is seemingly easy with use of a thermometer however the usual oral or tympanic thermometers become less accurate in truly cold patients and a central thermometer (rectal/ oesophageal / bladder) should be used. Signs and symptoms of moderate to severe hypothermia include: Shivering Reduced GCS and sluggish to fixed dilated pupils Bradycardia and hypotension Slow AF Hyperglycaemia AKI can develop if left untreated The ECG can be a clincher in the diagnosis before a temperature is gained and there are characteristic ECG findings that you should be aware of. A specific finding is the "J" or Osborn wave, a positive deflection at the J-point, seen below: 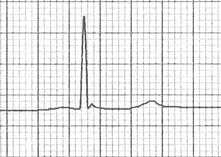 The height of the J wave is roughly proportional to the degree of hypothermia. Other ECG findings include: Prolonged PR, QRS and QT intervals Shivering artefact Ventricular ectopics Cardiac arrest due to VT, VF or asystole Below is an example of severe hypothermia demonstrating these features (temp 26 degrees) found on life in the fast lane. This ECG is very similar to a patient recently presenting unresponsive to the ED with a temp of 27'C. 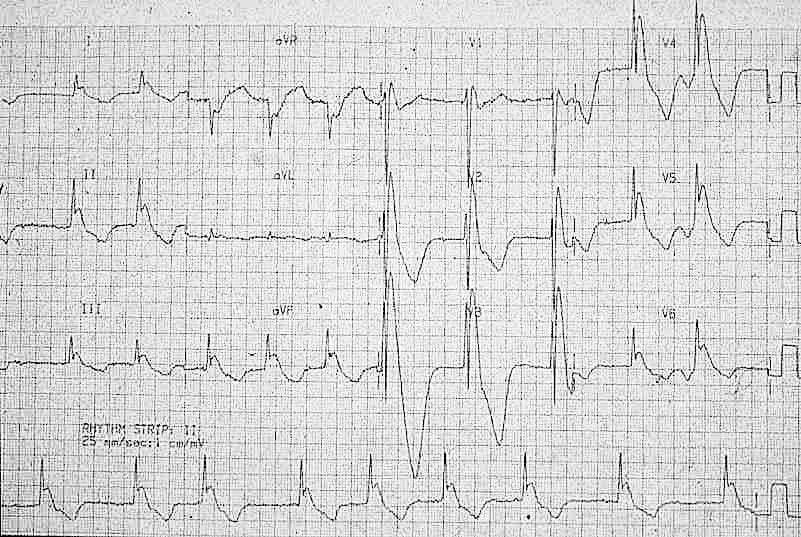 Management
Search for and treat secondary cause for hypothermia or leading to unprotected exposure to the cold (i.e sepsis, myxoedema, CVE, overdose, DKA etc). Rewarming strategies: Mild-moderate hypothermia Passive re-warming
Peripheral active re-warming
Severe hypothermia Central active warming
Be very careful transferring a hypothermic patient (particularly patients with temperatures <32'C) as moving the patient alone can trigger VF. Resuscitation Changes to ALS in a hypothermic arrest:
Further reading: https://litfl.com/hypothermia/ https://www.rcemlearning.co.uk/reference/hypothermia/ Martin Dore Dec 20
0 Comments
A patient presents to your department with worsening epigastric/chest pain after eating a chocolate bar. He felt a piece of the bar got stuck low down in his chest and he had been retching afterwards. His pain has been getting worse through the day and on arrival he is tachycardic, tachypneic and slightly hypoxic. He is able to swallow fluids, but despite large doses of IV morphine he remains uncomfortable. An arterial blood gas done by one of your colleagues shows mild type 2 respiratory failure and you are asked for advice. You go and review the patient and the investigations. Despite large doses of analgesia, the patient remains very uncomfortable and is reluctant to take deep breaths. On the CXR you note a subtle double line at the right side of the mediastinum and possible similar in the pericardium. See arrows on the CXR: 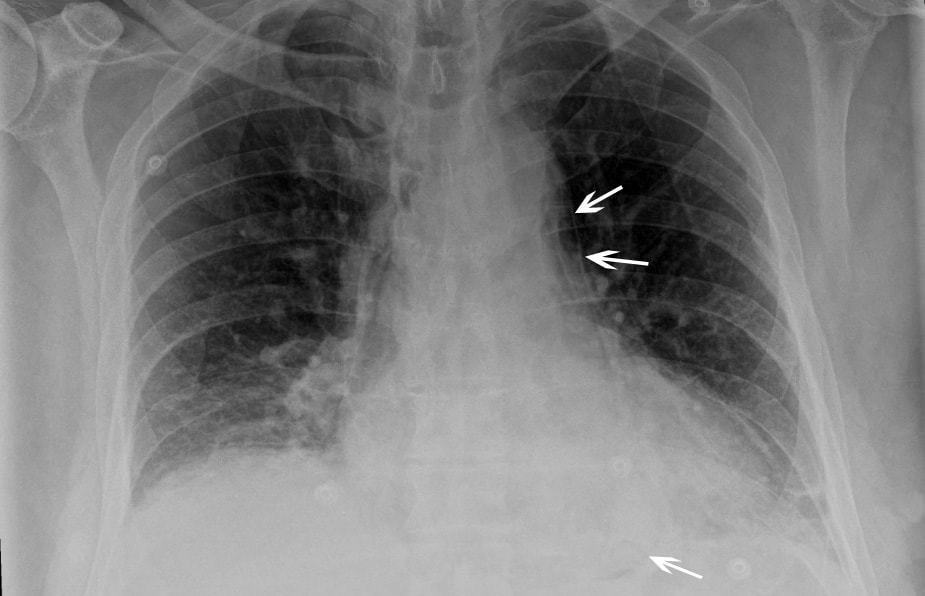 You suspect a pneumomediastinum and order a CT chest/abdomen +/- contrast. This confirms widespread mediastinal air suggestive of lower oesophageal perforation confirming your clinical suspicion of Boerhaave Syndrome. His hypoxia and type 2 respiratory failure can be explained by underventilating due to the severe pain.  CT image from the same patient, reported as: ‘Extensive pneumomediastinum, subcutaneous emphysema and bilateral pleural effusions with lower lobe consolidation. The appearance is suggestive of Boerhaave Syndrome.’ What is Boerhaave syndrome? Spontaneous rupture of the oesophagus, caused by forceful vomiting/retching. First described in 1724 by the Dutch physician Herman Boerhaave who diagnosed the condition in Jan van Wassenaer, a Grand Admiral of the Dutch Fleet who died 24hrs after vomiting, having feasted on a sumptuous meal with copious amounts of wine.* Pathophysiology: Spontaneous oesophageal rupture is caused by a sudden rise in internal oesophageal pressure produced during vomiting. The most common site of the perforation is in the lower third of the oesophagus. Symptoms: The classic triad of vomiting, chest pain and subcutaneous emphysema is only present in 14% of presentations. Other symptoms are upper abdominal pain, dyspnoea, tachypnea, odynophagia. The symptoms are often mistaken for other pathologies, e.g. myocardial infarction, chest infection. Diagnosis: is suspected on CXR by the presence of pneumomediastinum, and sometimes a pleural effusion and/or pneumothorax. A CT scan, ideally with contrast, will confirm the diagnosis. The diagnosis is often missed, and late presentations carry a high mortality. Prior to the advent of surgery the condition was universally lethal. Treatment is surgical intervention for most. Occasionally late presentations might be managed conservatively.
* Completely useless afternote: For the food lovers amongst you: his meal consisted of veal soup, cabbage boiled with mutton, calf sweetbreads, spinach, duck, two larks, apple compote, bread and beer. This was followed by Moselle wine, a dessert of pears, grapes and sweetbreads. No wonder he felt sick afterwards! Fred Declerck Nov 2020 Back pain and sciatica is very common presentation to the ED and the question of whether an MRI is required to rule out cauda equina syndrome always causes angst! Thankfully the Society for British Neurological Surgeons (SBNS) and British Association of Spinal Surgeons (BASS) have published guidance on when we should order an urgent MRI for these patients and it has been very nicely summarised into an infographic below: 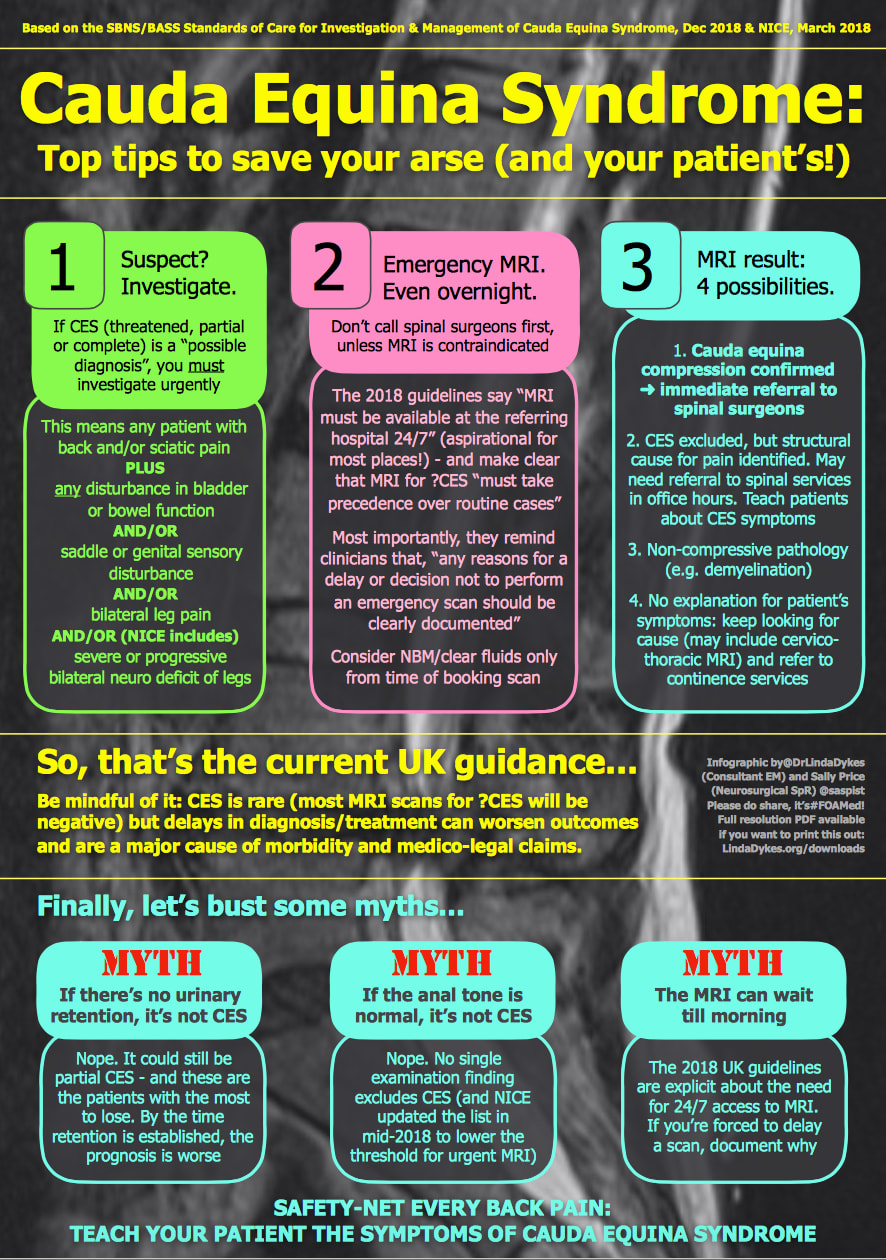 The full SBNS/BASS guideline can be accessed here: https://www.sbns.org.uk/index.php/policies-and-publications/ NICE have also published guidance on Sciatica (lumbar radiculopathy) which includes the back pain Red flags and can be found here: https://cks.nice.org.uk/topics/sciatica-lumbar-radiculopathy/ Martin Dore Nov 2020
|
This will be an archive of learning blogs and lunchtime learnings bites!
Archives
February 2023
Categories
All
|
 RSS Feed
RSS Feed