|
https://litfl.com/vt-versus-svt-ecg-library/
LIfe in the Fast Lane blog looking at ways to decide if your patient has a VT or and SVT. Ryan/Fordham Dec 2021
0 Comments
A patient presented with an LVAD (Left ventricular assist device), thankfully the patient was well, but many questions were asked regarding what we would do if the patient was unwell. An LVAD is a device that is implanted in patients with end stage heart failure, often as a bridge to heart transplantation. The device acts as a pump for the heart and assists cardiac output, with the pump working correctly these patients will be well perfused but may not have a pulse. Patients with these devices are rare but present a unique challenge when presenting with an LVAD emergency. Life threatening LVAD emergences include device failure, stroke, bleeding, LVAD thrombosis and systemic infection. National guidelines on the management of patients with these devices are scarce however there is a really helpful article in the EMJ, published by C.Bowels et al in 2017 which is definitely worth a read. Here are the suggested algorithms from the article for an unwell patient with an LVAD: 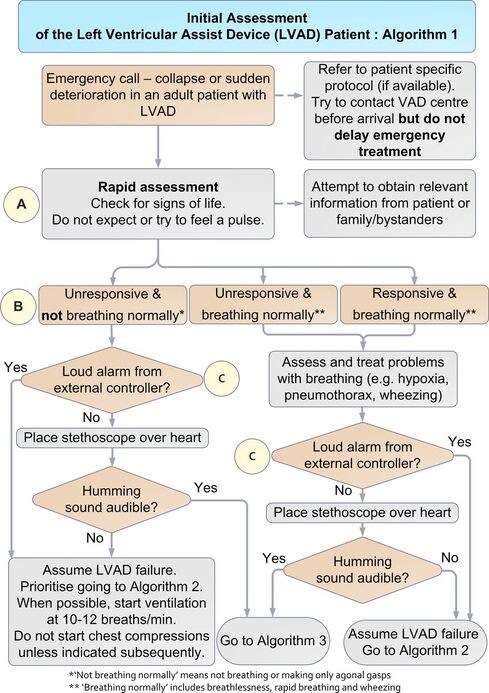 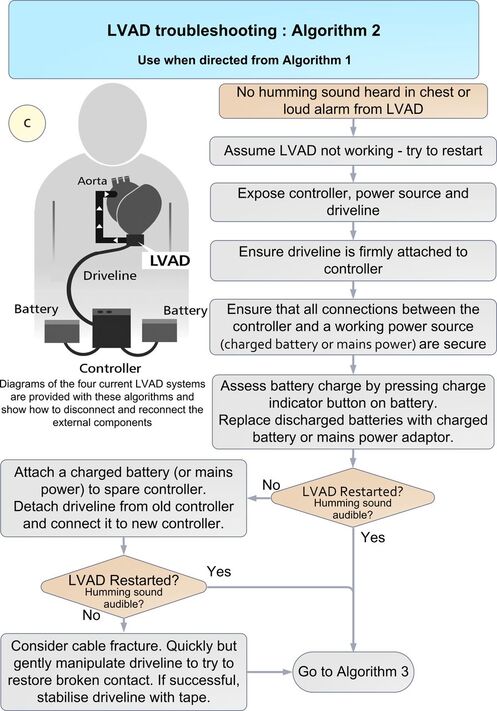 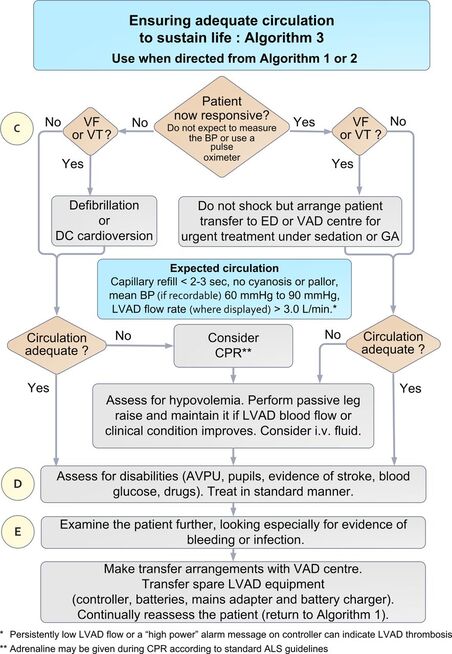 The article can be accessed Here
Bowles CT, Hards R, Wrightson N, et al. Algorithms to guide ambulance clinicians in the management of emergencies in patients with implanted rotary left ventricular assist devices. EMJ 2017;34:842-8 The are a number of studies in the literature looking at the value of the ECG after an Out of Hospital Cardiac Arrest with ROSC.
Circ Cardiovasc Interv. 2015;8:e002784. DOI: 10.1161/CIRCINTERVENTIONS.115.002784. This 2015 paper looked at 210 Patients who had ROSC after an out of hospital cardiac arrest. The post arrest ECG was classified into 3 main groups. 1) ST elevation or presumably new left bundle branch block (2) Other ECG signs indicating myocardial ischaemia (3) No ECG signs indicating myocardial ischaemia. Coronary Angiography findings were then correlated with the ECG findings. Notable findings were: 1) Mean age 62 +/- 12 years 2) 6 Month survival with good neurological outcome 54% 3) STEMI or presumed new LBBB identified patients with reduced TIMI flow with sensitivity 70%, specificity 62%. 4) An acute coronary occlusion was found in 11% of patients in group (3), those with a post resuscitation ecg showing no signs of Myocardial Ischaemia. 5) 32% of patients with initial non shockable rhythms had significantly reduced TIMI flow at angiography. What does this tell us? After initial resuscitation of the patient with an Out of Hospital Cardiac Arrest consider carefully the need for Emergency PCI even if the ecg shows no ischaemia. Want to read more? https://rebelem.com/the-difoccult-trial-time-to-change-from-stemi-nstemi-to-omi-nomi/ This October 2020 paper and post highlighted by Nick Pocock proposes a new way of thinking in Post Cardiac Arrest Care. Steve Fordham November 2020 Syncope is a very common presentation to the ED. The ECG is a vital investigation in the context of a transient loss of consciousness / syncope as it can identify the cause, including rare conditions that can lead to sudden cardiac death. The pneumonic WOBBLER can be used as a useful way of asessing the ECG in this context with consideration for these rare causes. W - Wolff-Parkinson-White syndrome – A short PR interval and delta wave:  O - Obstructed AV pathway – look for 2nd or 3rd degree block: 2nd degree block: Mobitz type 1 - PR prolongs then QRS not present: 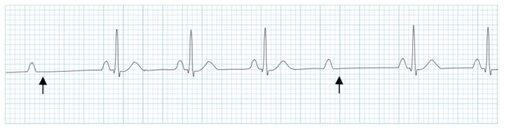 Mobitz 2 - PR Is constant but QRS randomly not present: 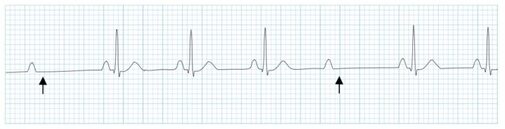 3rd Degree block - complete dissociation between P waves and QRS complexes: 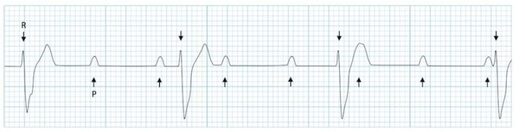 B - Bifascicular block - The combination of axis deviation and right bundle branch block: Bifasicular block has a low risk of deteriorating into complete heart block (~ 1% per year) but trifasicular block (Axis deviation, RBBB and prolonged PR) has a greater risk. B - Brugada - Coved ST elevation (shark fin) followed by a negative T wave in V1-V3 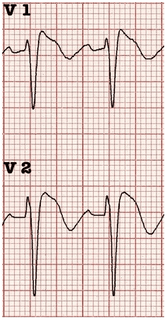 L – Left ventricular hypertrophy - Consider Aortic stenosis and Hypertrophic Obstructive cardiomyopathy (HOCM), these can present with exertional syncope.  LVH diagnostic criteria - S wave in V2 + R wave in V5 > 35 mm E – Epsilon wave - A feature of Arrythmogenic right ventricular dysplasia (ARVD). This is another rare cause of sudden cardiac arrest. The epsilon wave looks a bit like the J wave of hypothermia and may be associated with T wave inversion in V1-V3:  R - Repolarisation abnormality, such as long or Short QT syndrome.
A prolonged QT is > 440ms in men or > 460ms in women. A QT >500ms is associated with increased risk of Torsades de pointes. A QT of <350ms is abnormally short. So thats it, next time you see a patient with a transient loss of consiousness make sure thier ECG is not a WOBBLER. Dr Martin Dore The 3 P's of an uncomplicated faint
Transient loss of consciousness (TLoC) is common but can be a daunting presentation in ED. NICE recommends a simple faint if there are no red flags for cardiac syncope and the 3 P's are present: Posture - prolonged standing Prodrome - sweating or feeling warm/hot before transient loss of conciousness, pallor Provoking factors - pain, medical procedure RED FLAGS
We have recently updated the departmental chest pain pathway. When a patient presents with chest pain suspicious for cardiac ischaemia an ECG should be performed immediately. Not all patients with critical ischaemia present with ST-Elevation on their ECG. The ECG patterns below are STEMI equivalents and if found in a patient with the right clinical presentation should prompt an urgent senior review with early discussion with cardiology. 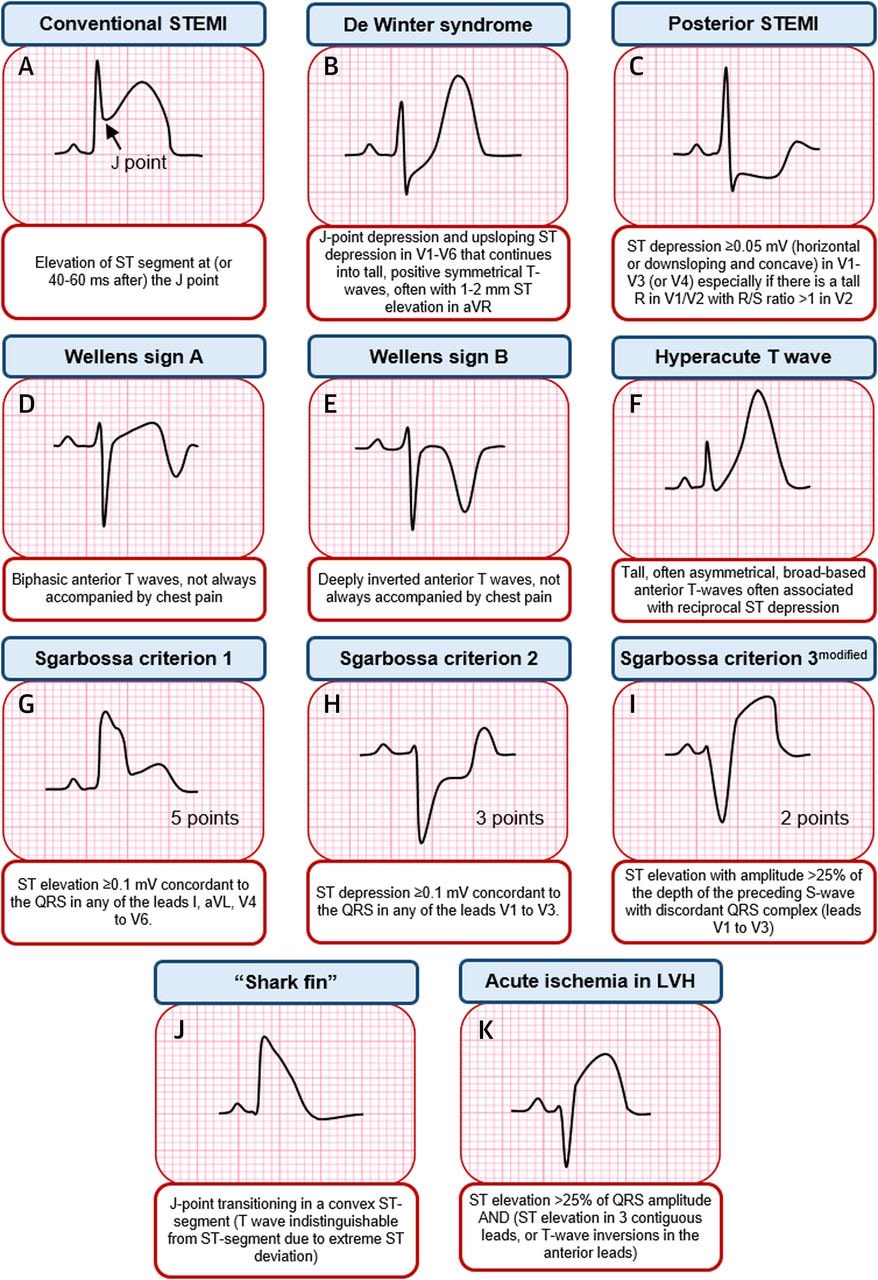 Source: Asatryan B et al,Electrocardiographic diagnosis of life threatening STEMI Equivalents, JACC:case reports, 2019, 1(4)
Dr Martin Dore |
This will be an archive of learning blogs and lunchtime learnings bites!
Archives
February 2023
Categories
All
|
 RSS Feed
RSS Feed