|
Unfortunately the supply of Diamorphine has been challenging over recent months and at times our stock has ran out. Although it is fantastic drug to treat children with moderate to severe pain there is an alternative that it just as good - INTRANASAL FENTANYL We have a new departmental guideline on the use of IN fentanyl on the tree of knowledge under Anaesthetics/sedation analgesia. The Key points can be found below: 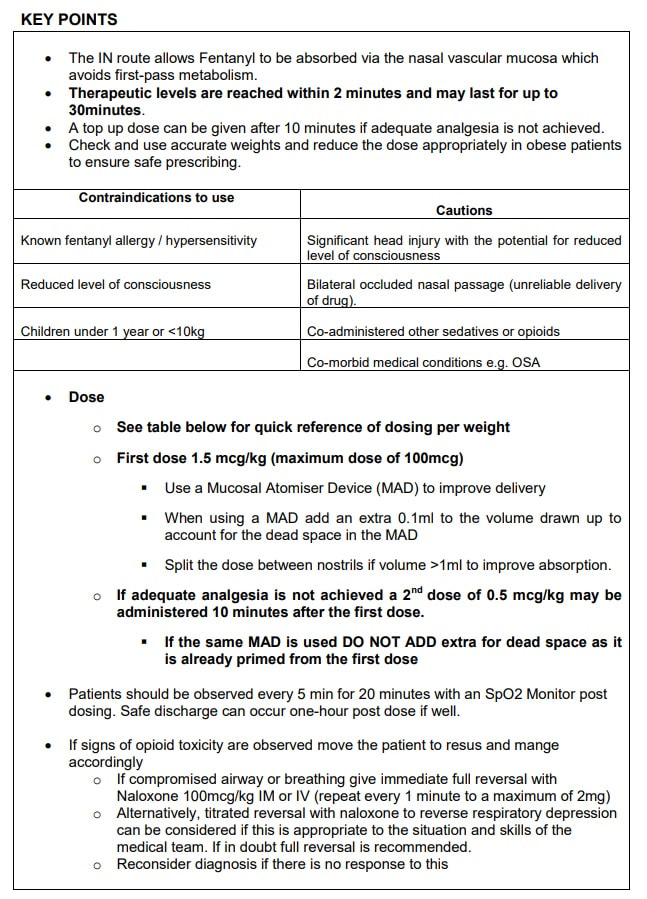 Martin Dore 17/02/22
0 Comments
Yvette highlighted a change to management for skin tears. Please see the flow diagram below (this poster can be found around the department): 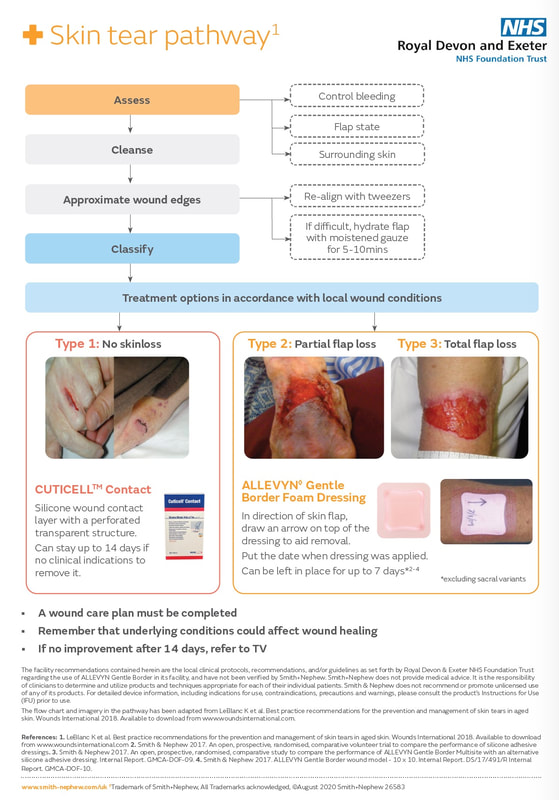 Additional resourcesVideo on how to apply a zimmer splint (dorsal blocking splint) HERE
Don't forget the bubbles have a fantastic blog post on finger injuries in 2 parts (hyperlinks below), Its a paediatric blog but the learning is transferrable to adult injuries. Part 1 - Basics and bones Part 2 - Tendons and ligaments Jo Mclaughlin March 2021 Back pain and sciatica is very common presentation to the ED and the question of whether an MRI is required to rule out cauda equina syndrome always causes angst! Thankfully the Society for British Neurological Surgeons (SBNS) and British Association of Spinal Surgeons (BASS) have published guidance on when we should order an urgent MRI for these patients and it has been very nicely summarised into an infographic below: 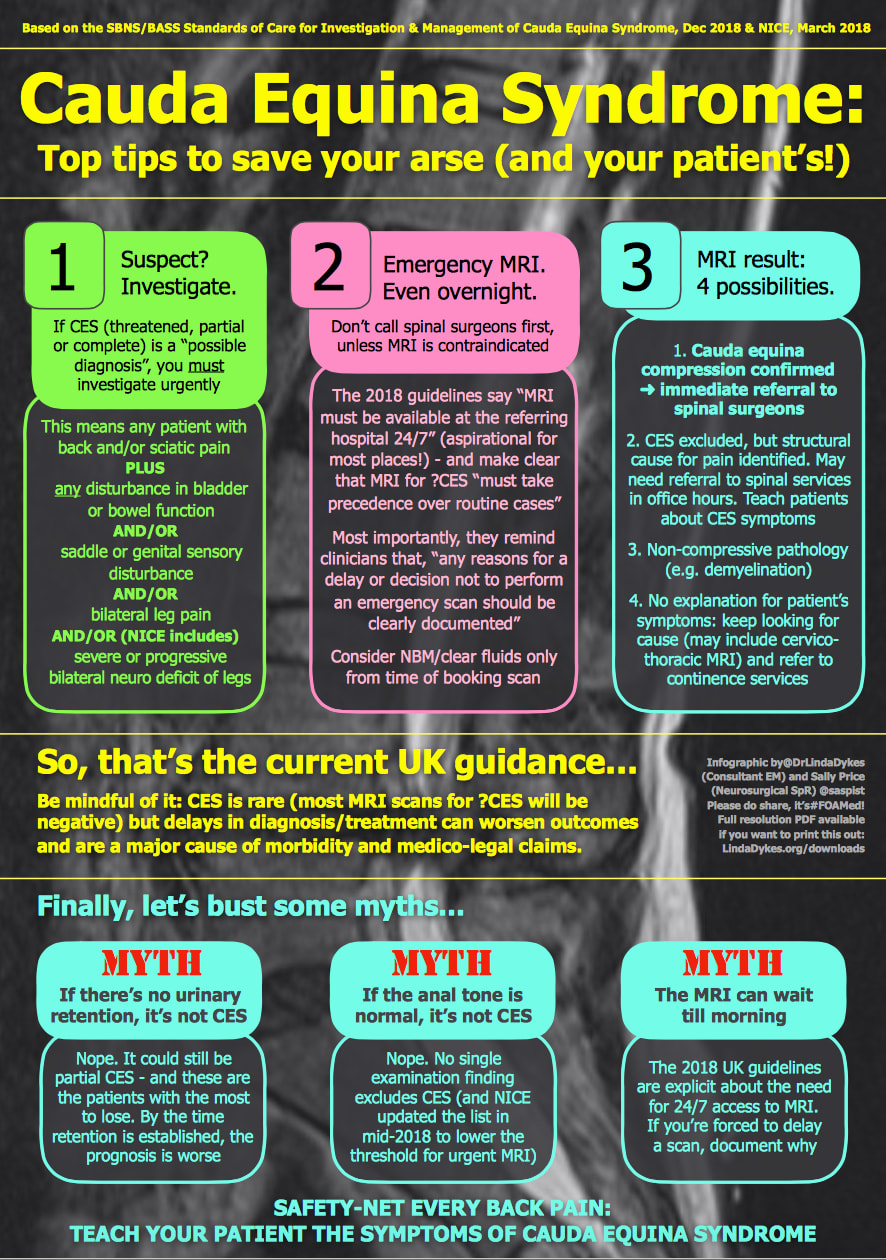 The full SBNS/BASS guideline can be accessed here: https://www.sbns.org.uk/index.php/policies-and-publications/ NICE have also published guidance on Sciatica (lumbar radiculopathy) which includes the back pain Red flags and can be found here: https://cks.nice.org.uk/topics/sciatica-lumbar-radiculopathy/ Martin Dore Nov 2020
The Ossification centres of the paediatric elbow Xray can cause confusion. Is that normal or is there a fracture? is a common question in this age group. If you remember CRITOE you'll be better prepared! CRITOE refers to the order these ossification centres appear on the Xray. The year of ossification can vary slightly but they always appear in the same order: Capitellum - 1yr (age visible on the Xray) Radial head - 3yrs Internal epicondyl - 5 yrs Trochlear - 7yrs Olecranon - 9yrs External epichondyl - 11 yrs 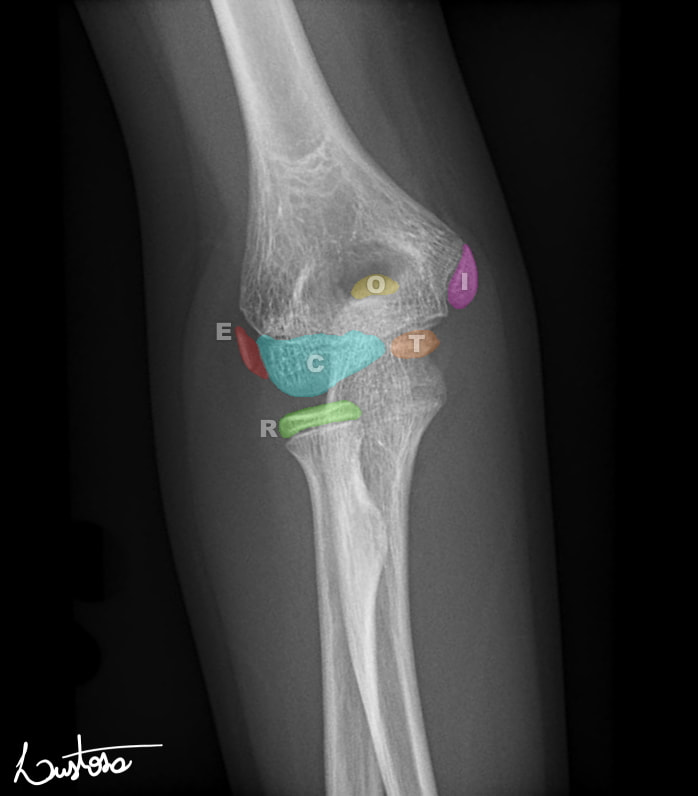 Case courtesy of Leonardo Lustosa, <a href="https://radiopaedia.org/">Radiopaedia.org</a>. From the case <a href="https://radiopaedia.org/cases/80555">rID: 80555</a> Why is this important? Knowing the order will allow you to see if there is an ossification centre missing, i.e it may have avulsed and may be hidden in the Xray. If for example you can see the ossification centre of the trochlear or the olecranon but cannot see the internal epicondyl be very suspicious of an avulsion of the internal epicondyl. The video below from Radiopaedia explains this in greater depth. Martin Dore Nov 2020
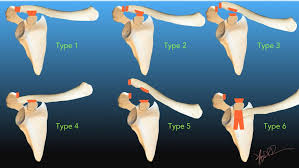 The Rockwood Grading for AcromioClavicular Joint injuries is from 1 to 6.(1) In Grade 1 to 3 there is a varying degree of injury to the AcromioClavicular Ligaments (AC) and the CoracoClavicular ligaments (CC). Radiographically this translates into a 25-100% CoracoClavicular (CC) distance. For Grade 4-6 the disruption of the AC and CC ligaments and the Deltopectoral Fascia is more severe. For Grade 5 the CC distance is >100% of normal. (2) 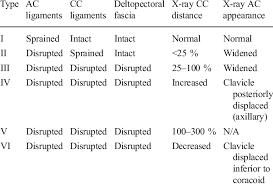 Grade 1-3 Injuries can be managed conservatively with a Broad Arm Sling, Analgesia, an Advice Sheet and discharge. The orthopaedic referral chart (Accessed Oct 2020) states between 0830-2200 Grade 4-6 Injuries should be discussed with the Orthopaedic team on call and between 2200-0830 discussion is not indicated but a fracture clinic triage should be completed. Please ensure Senior ED discussion for all Grade 4-6 Injuries and especially if there is any suspicion of Major Mechanism, Open Injury or Neurovascular Compromise. Ref1. https://faculty.washington.edu/jeff8rob/trauma-radiology-reference-resource/9-upper-extremity/rockwood-classification-of-acromioclavicular-joint-separation/ Ref2. https://www.researchgate.net/figure/Rockwood-classification-of-acromioclavicular-injuries_tbl1_272096166 Steve Fordham Oct 2020 Tetanus is an infection caused by the anaerobic bacteria clostridium tetani which is found in soil and manure. Tetanus infection has a 90% mortality, but thankfully due to the success of vaccinations, it is rare with only 4 cases in the UK in 2019. Patients often rock up to ED because someone told them they “might need a tetanus” and the guidelines have recently changed as to who needs a booster/immunoglobulin, so hopefully this little 5 step plan should demystify it for you! STEP 1: ASSESS THE WOUND:
Tetanus-prone:
Tetanus high risk wound: is any of the above PLUS
Clean:
Note - A wound can't be tetanus high risk unless its already tetanus prone Remember that ALL wounds require thorough washout with clean water or normal saline. STEP 2: WHATS THE PATIENTS IMMUNISATION STATUS? So now you know what category the patients wound is in, the next question is whats the patient's immunisation status! Remember a full Course of tetanus vaccinations is 5 doses. A ‘priming course’ means 3 doses which is given in childhood. The table below is from the ‘green book’ on tetanus, simplified below: 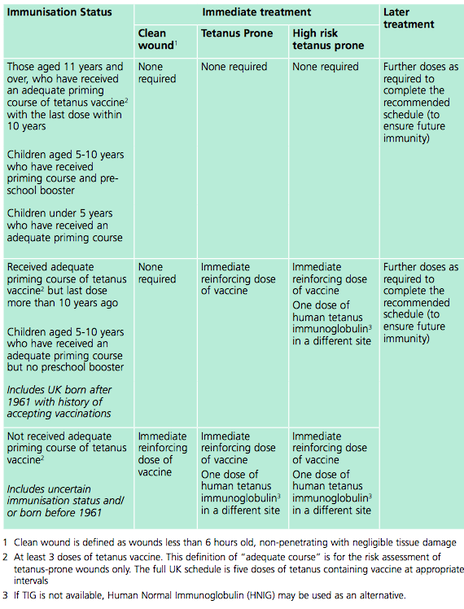 IN SIMPLER TERMS:
The main change in the guidance is that any adult who hasn't had a booster for 10 years with a tetanus prone wound now needs a booster! It used to be that if you'd had your full childhood immunisations then this wasn't indicated, so make sure your patient knows when their last booster was! STEP 3: WHAT DOSE DO I PRESCRIBE?: Tetanus Booster: Revaxis is the name of the tetanus booster and is a 3 in 1 diphtheria, tetanus + polio vaccine. Give one 0.5ml syringe. Immunoglobulin: For most cases 250 iu by IM injection If >24 hours have elapsed since the injury, or there is a risk of heavy contamination or burns then 500iu by IM injection. STEP 4: WHERE DO I FIND IT IN ED?: Tetanus booster- This is called ‘Revaxis’ and lives in the drugs fridge in resus. Attach a green needle directly to the syringe and its ready to be given IM! There’s a small sticker with a barcode on the side of the syringe which you should stick on the ED card next to where you sign for giving the drug. Tetanus immunoglobulin – This is technically a ‘blood product’ in the trust. Which means that you need to call blood bank and inform them that your patient needs immunoglobulin and have their details handy and the dose you require. When the tetanus is ready it will be available for the nurses to see on ‘blood track’ and they need to print a pick up slip to take to pick it up. This usually takes about 20-30 minutes. Doctors cannot pick this up, but can give the injection if you have a barcode for the blood transfusion machine. When you have the immunoglobulin you need to print the patient a wrist band and take the blood transfusion scanning machine with you to the patient – doing an ID check and scanning the square barcode on the side of the immunoglobulin (if you do not do this the lab will call up and will ask you to!) What if I need to give a booster AND Immunoglobulin? – inject IM in two different sites- i.e.:one arm each. STEP 5: ONGOING CARE:
References: The very long full government guidelines on tetanus immunisations: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/859519/Greenbook_chapter_30_Tetanus_January_2020.pdf Dr Alice Hunter |
This will be an archive of learning blogs and lunchtime learnings bites!
Archives
February 2023
Categories
All
|
 RSS Feed
RSS Feed