|
RCEM 2022 Guideline
Summary of Recommendations 1. All Emergency Departments (EDs) should be familiar with the term Acute Behavioural Disturbance (ABD) and the recognition of potential cases. 2. All EDs should have a locally agreed strategy for the management of cases of ABD. 3. All EDs should have an identified area suitable to provide verbal and environmental de-escalation of ABD cases when required. 4. All EDs should have 24/7 access to sufficient security staff to provide support. These staff should be appropriately trained to provide additional de-escalation and where appropriate, restraint of patients to support clinical care. Where this is not provided, the Trust should clearly describe any alternative provision and how this fulfils the requirements of the Health and Safety at Work Act 1974. 5. Early sedation should be considered in severe cases of ABD, including where prolonged activity or restraint has taken place. 6. In most cases of ABD requiring parenteral sedation, intramuscular ketamine or droperidol are recommended agents. https://rcem.ac.uk/wp-content/uploads/2022/01/Acute_Behavioural_Disturbance_Final.pdf Steve Fordham Feb 2022
0 Comments
A brief PowerPoint presentation on the pathology and management of patients with Cyanide poisoning.
Uploaded 10/3/2021 by Lewis Jones Winter has finally arrived and a new season brings new environmental factors that may play a part in a patients presentation. As we move into the coldest months of the year the identification and management of hypothermia is something which we may all need to revise. Hypothermia can be categorised into: Mild - 32-35'C Moderate- 28 - 32'C Severe - less than 28'C In these cold months be sure to consider hypothermia in elderly patients and the young when presenting acutely unwell. The identification of hypothermia is seemingly easy with use of a thermometer however the usual oral or tympanic thermometers become less accurate in truly cold patients and a central thermometer (rectal/ oesophageal / bladder) should be used. Signs and symptoms of moderate to severe hypothermia include: Shivering Reduced GCS and sluggish to fixed dilated pupils Bradycardia and hypotension Slow AF Hyperglycaemia AKI can develop if left untreated The ECG can be a clincher in the diagnosis before a temperature is gained and there are characteristic ECG findings that you should be aware of. A specific finding is the "J" or Osborn wave, a positive deflection at the J-point, seen below: 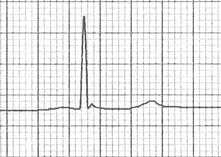 The height of the J wave is roughly proportional to the degree of hypothermia. Other ECG findings include: Prolonged PR, QRS and QT intervals Shivering artefact Ventricular ectopics Cardiac arrest due to VT, VF or asystole Below is an example of severe hypothermia demonstrating these features (temp 26 degrees) found on life in the fast lane. This ECG is very similar to a patient recently presenting unresponsive to the ED with a temp of 27'C. 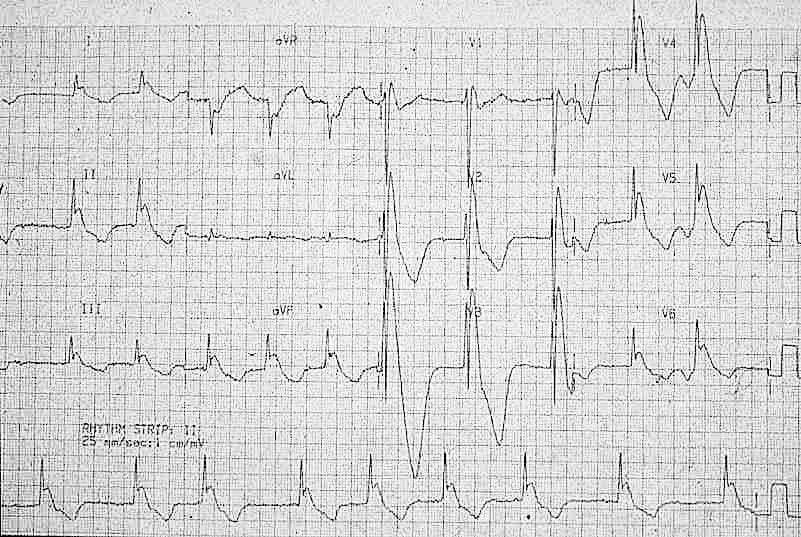 Management
Search for and treat secondary cause for hypothermia or leading to unprotected exposure to the cold (i.e sepsis, myxoedema, CVE, overdose, DKA etc). Rewarming strategies: Mild-moderate hypothermia Passive re-warming
Peripheral active re-warming
Severe hypothermia Central active warming
Be very careful transferring a hypothermic patient (particularly patients with temperatures <32'C) as moving the patient alone can trigger VF. Resuscitation Changes to ALS in a hypothermic arrest:
Further reading: https://litfl.com/hypothermia/ https://www.rcemlearning.co.uk/reference/hypothermia/ Martin Dore Dec 20 |
This will be an archive of learning blogs and lunchtime learnings bites!
Archives
February 2023
Categories
All
|
 RSS Feed
RSS Feed