|
Syncope is a very common presentation to the ED. The ECG is a vital investigation in the context of a transient loss of consciousness / syncope as it can identify the cause, including rare conditions that can lead to sudden cardiac death. The pneumonic WOBBLER can be used as a useful way of asessing the ECG in this context with consideration for these rare causes. W - Wolff-Parkinson-White syndrome – A short PR interval and delta wave: 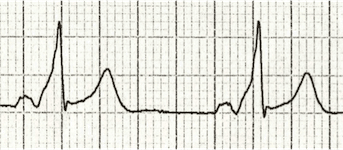 O - Obstructed AV pathway – look for 2nd or 3rd degree block: 2nd degree block: Mobitz type 1 - PR prolongs then QRS not present: 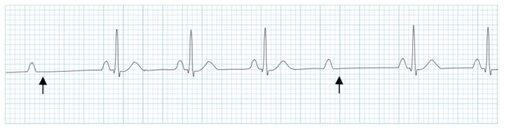 Mobitz 2 - PR Is constant but QRS randomly not present: 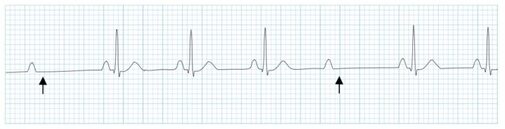 3rd Degree block - complete dissociation between P waves and QRS complexes: 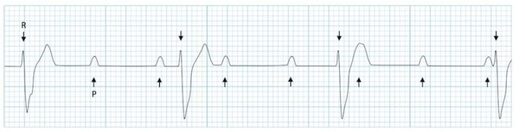 B - Bifascicular block - The combination of axis deviation and right bundle branch block: Bifasicular block has a low risk of deteriorating into complete heart block (~ 1% per year) but trifasicular block (Axis deviation, RBBB and prolonged PR) has a greater risk. B - Brugada - Coved ST elevation (shark fin) followed by a negative T wave in V1-V3 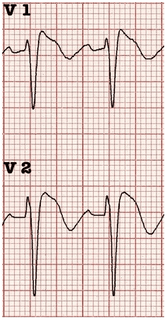 L – Left ventricular hypertrophy - Consider Aortic stenosis and Hypertrophic Obstructive cardiomyopathy (HOCM), these can present with exertional syncope.  LVH diagnostic criteria - S wave in V2 + R wave in V5 > 35 mm E – Epsilon wave - A feature of Arrythmogenic right ventricular dysplasia (ARVD). This is another rare cause of sudden cardiac arrest. The epsilon wave looks a bit like the J wave of hypothermia and may be associated with T wave inversion in V1-V3: 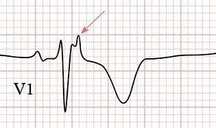 R - Repolarisation abnormality, such as long or Short QT syndrome.
A prolonged QT is > 440ms in men or > 460ms in women. A QT >500ms is associated with increased risk of Torsades de pointes. A QT of <350ms is abnormally short. So thats it, next time you see a patient with a transient loss of consiousness make sure thier ECG is not a WOBBLER. Dr Martin Dore
0 Comments
|
This will be an archive of learning blogs and lunchtime learnings bites!
Archives
February 2023
Categories
All
|
 RSS Feed
RSS Feed