|
Winter has finally arrived and a new season brings new environmental factors that may play a part in a patients presentation. As we move into the coldest months of the year the identification and management of hypothermia is something which we may all need to revise. Hypothermia can be categorised into: Mild - 32-35'C Moderate- 28 - 32'C Severe - less than 28'C In these cold months be sure to consider hypothermia in elderly patients and the young when presenting acutely unwell. The identification of hypothermia is seemingly easy with use of a thermometer however the usual oral or tympanic thermometers become less accurate in truly cold patients and a central thermometer (rectal/ oesophageal / bladder) should be used. Signs and symptoms of moderate to severe hypothermia include: Shivering Reduced GCS and sluggish to fixed dilated pupils Bradycardia and hypotension Slow AF Hyperglycaemia AKI can develop if left untreated The ECG can be a clincher in the diagnosis before a temperature is gained and there are characteristic ECG findings that you should be aware of. A specific finding is the "J" or Osborn wave, a positive deflection at the J-point, seen below: 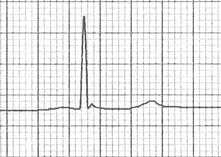 The height of the J wave is roughly proportional to the degree of hypothermia. Other ECG findings include: Prolonged PR, QRS and QT intervals Shivering artefact Ventricular ectopics Cardiac arrest due to VT, VF or asystole Below is an example of severe hypothermia demonstrating these features (temp 26 degrees) found on life in the fast lane. This ECG is very similar to a patient recently presenting unresponsive to the ED with a temp of 27'C. 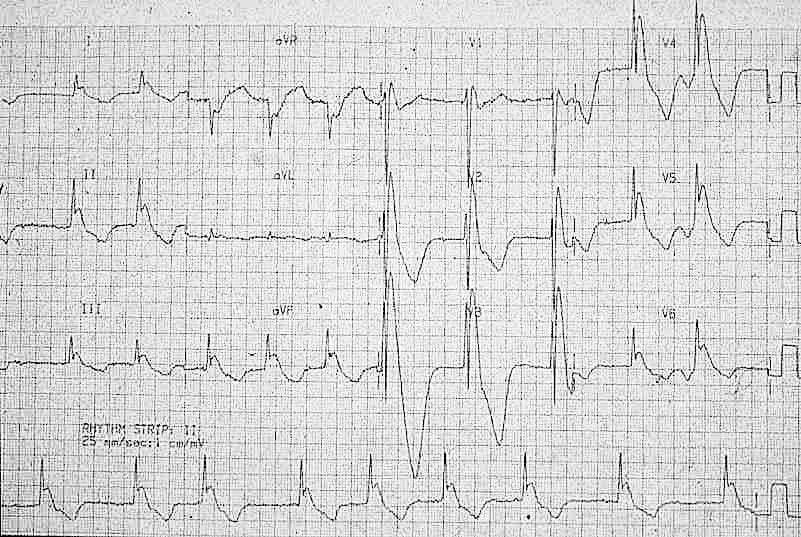 Management
Search for and treat secondary cause for hypothermia or leading to unprotected exposure to the cold (i.e sepsis, myxoedema, CVE, overdose, DKA etc). Rewarming strategies: Mild-moderate hypothermia Passive re-warming
Peripheral active re-warming
Severe hypothermia Central active warming
Be very careful transferring a hypothermic patient (particularly patients with temperatures <32'C) as moving the patient alone can trigger VF. Resuscitation Changes to ALS in a hypothermic arrest:
Further reading: https://litfl.com/hypothermia/ https://www.rcemlearning.co.uk/reference/hypothermia/ Martin Dore Dec 20
0 Comments
A patient presents to your department with worsening epigastric/chest pain after eating a chocolate bar. He felt a piece of the bar got stuck low down in his chest and he had been retching afterwards. His pain has been getting worse through the day and on arrival he is tachycardic, tachypneic and slightly hypoxic. He is able to swallow fluids, but despite large doses of IV morphine he remains uncomfortable. An arterial blood gas done by one of your colleagues shows mild type 2 respiratory failure and you are asked for advice. You go and review the patient and the investigations. Despite large doses of analgesia, the patient remains very uncomfortable and is reluctant to take deep breaths. On the CXR you note a subtle double line at the right side of the mediastinum and possible similar in the pericardium. See arrows on the CXR: 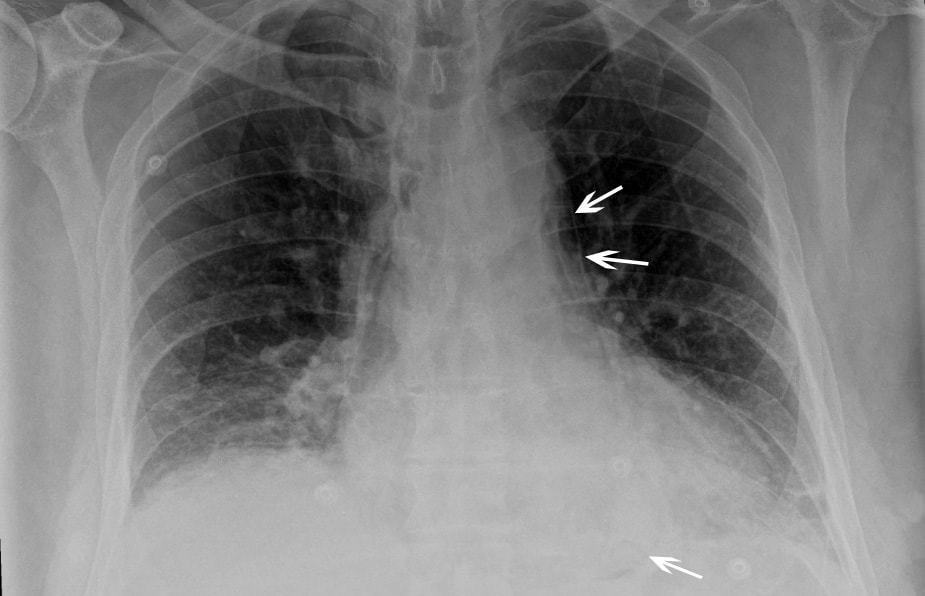 You suspect a pneumomediastinum and order a CT chest/abdomen +/- contrast. This confirms widespread mediastinal air suggestive of lower oesophageal perforation confirming your clinical suspicion of Boerhaave Syndrome. His hypoxia and type 2 respiratory failure can be explained by underventilating due to the severe pain.  CT image from the same patient, reported as: ‘Extensive pneumomediastinum, subcutaneous emphysema and bilateral pleural effusions with lower lobe consolidation. The appearance is suggestive of Boerhaave Syndrome.’ What is Boerhaave syndrome? Spontaneous rupture of the oesophagus, caused by forceful vomiting/retching. First described in 1724 by the Dutch physician Herman Boerhaave who diagnosed the condition in Jan van Wassenaer, a Grand Admiral of the Dutch Fleet who died 24hrs after vomiting, having feasted on a sumptuous meal with copious amounts of wine.* Pathophysiology: Spontaneous oesophageal rupture is caused by a sudden rise in internal oesophageal pressure produced during vomiting. The most common site of the perforation is in the lower third of the oesophagus. Symptoms: The classic triad of vomiting, chest pain and subcutaneous emphysema is only present in 14% of presentations. Other symptoms are upper abdominal pain, dyspnoea, tachypnea, odynophagia. The symptoms are often mistaken for other pathologies, e.g. myocardial infarction, chest infection. Diagnosis: is suspected on CXR by the presence of pneumomediastinum, and sometimes a pleural effusion and/or pneumothorax. A CT scan, ideally with contrast, will confirm the diagnosis. The diagnosis is often missed, and late presentations carry a high mortality. Prior to the advent of surgery the condition was universally lethal. Treatment is surgical intervention for most. Occasionally late presentations might be managed conservatively.
* Completely useless afternote: For the food lovers amongst you: his meal consisted of veal soup, cabbage boiled with mutton, calf sweetbreads, spinach, duck, two larks, apple compote, bread and beer. This was followed by Moselle wine, a dessert of pears, grapes and sweetbreads. No wonder he felt sick afterwards! Fred Declerck Nov 2020 Back pain and sciatica is very common presentation to the ED and the question of whether an MRI is required to rule out cauda equina syndrome always causes angst! Thankfully the Society for British Neurological Surgeons (SBNS) and British Association of Spinal Surgeons (BASS) have published guidance on when we should order an urgent MRI for these patients and it has been very nicely summarised into an infographic below: 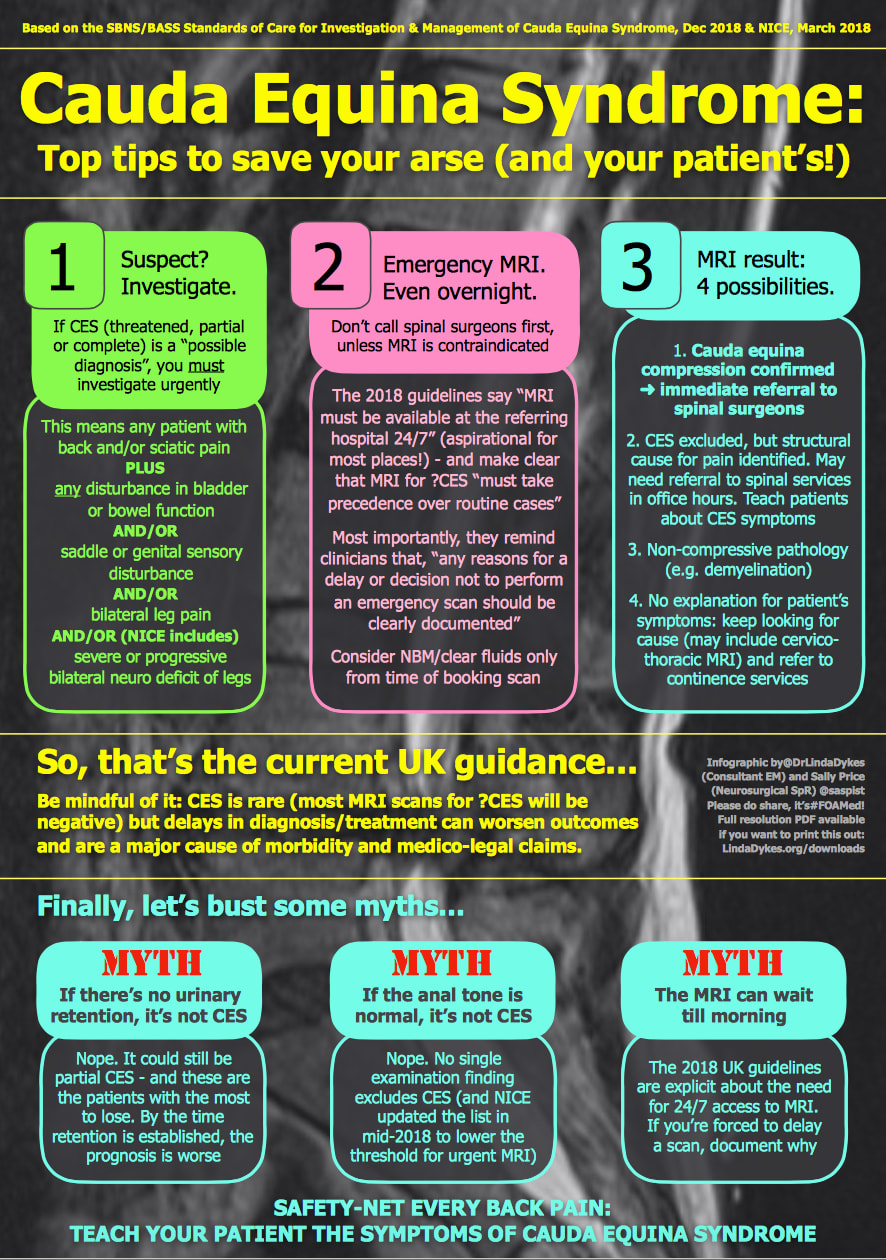 The full SBNS/BASS guideline can be accessed here: https://www.sbns.org.uk/index.php/policies-and-publications/ NICE have also published guidance on Sciatica (lumbar radiculopathy) which includes the back pain Red flags and can be found here: https://cks.nice.org.uk/topics/sciatica-lumbar-radiculopathy/ Martin Dore Nov 2020
The Ossification centres of the paediatric elbow Xray can cause confusion. Is that normal or is there a fracture? is a common question in this age group. If you remember CRITOE you'll be better prepared! CRITOE refers to the order these ossification centres appear on the Xray. The year of ossification can vary slightly but they always appear in the same order: Capitellum - 1yr (age visible on the Xray) Radial head - 3yrs Internal epicondyl - 5 yrs Trochlear - 7yrs Olecranon - 9yrs External epichondyl - 11 yrs 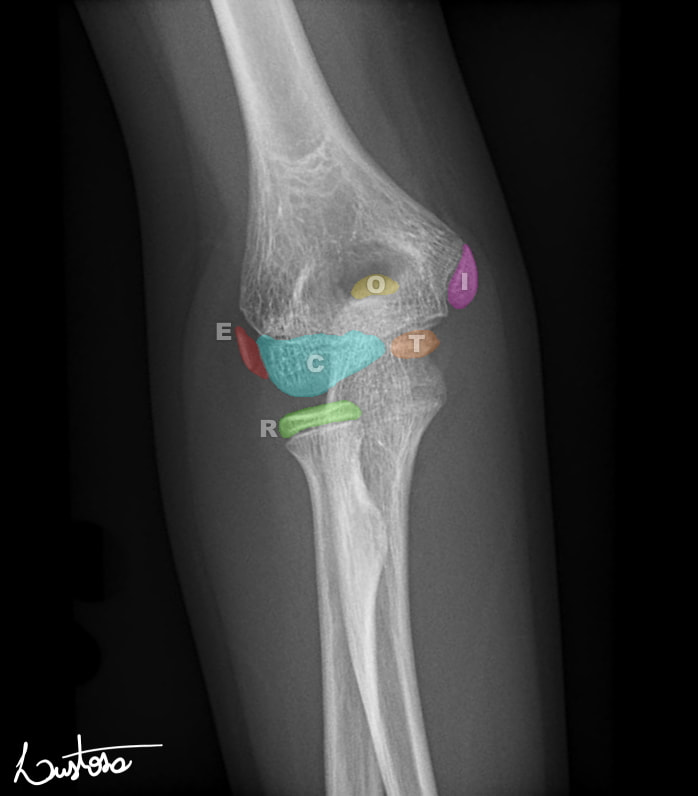 Case courtesy of Leonardo Lustosa, <a href="https://radiopaedia.org/">Radiopaedia.org</a>. From the case <a href="https://radiopaedia.org/cases/80555">rID: 80555</a> Why is this important? Knowing the order will allow you to see if there is an ossification centre missing, i.e it may have avulsed and may be hidden in the Xray. If for example you can see the ossification centre of the trochlear or the olecranon but cannot see the internal epicondyl be very suspicious of an avulsion of the internal epicondyl. The video below from Radiopaedia explains this in greater depth. Martin Dore Nov 2020
A 41 year old patient presents following and Out Of Hospital Cardiac Arrest. His identity is unknown but the ambulance service do bring his I-Phone with him. Click the Emergency button on the bottom of the locked home screen then click *Medical ID on the bottom of the next screen.  Have you updated your own phone? Click Emergency SOS in the settings Menu, then click Edit Emergency Contacts in Health in the next menu and fill in your ICE details. 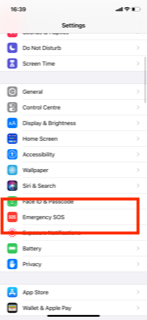 Steve Fordham, November 2020
The are a number of studies in the literature looking at the value of the ECG after an Out of Hospital Cardiac Arrest with ROSC.
Circ Cardiovasc Interv. 2015;8:e002784. DOI: 10.1161/CIRCINTERVENTIONS.115.002784. This 2015 paper looked at 210 Patients who had ROSC after an out of hospital cardiac arrest. The post arrest ECG was classified into 3 main groups. 1) ST elevation or presumably new left bundle branch block (2) Other ECG signs indicating myocardial ischaemia (3) No ECG signs indicating myocardial ischaemia. Coronary Angiography findings were then correlated with the ECG findings. Notable findings were: 1) Mean age 62 +/- 12 years 2) 6 Month survival with good neurological outcome 54% 3) STEMI or presumed new LBBB identified patients with reduced TIMI flow with sensitivity 70%, specificity 62%. 4) An acute coronary occlusion was found in 11% of patients in group (3), those with a post resuscitation ecg showing no signs of Myocardial Ischaemia. 5) 32% of patients with initial non shockable rhythms had significantly reduced TIMI flow at angiography. What does this tell us? After initial resuscitation of the patient with an Out of Hospital Cardiac Arrest consider carefully the need for Emergency PCI even if the ecg shows no ischaemia. Want to read more? https://rebelem.com/the-difoccult-trial-time-to-change-from-stemi-nstemi-to-omi-nomi/ This October 2020 paper and post highlighted by Nick Pocock proposes a new way of thinking in Post Cardiac Arrest Care. Steve Fordham November 2020 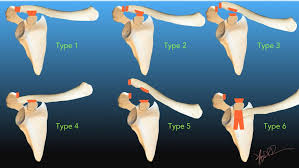 The Rockwood Grading for AcromioClavicular Joint injuries is from 1 to 6.(1) In Grade 1 to 3 there is a varying degree of injury to the AcromioClavicular Ligaments (AC) and the CoracoClavicular ligaments (CC). Radiographically this translates into a 25-100% CoracoClavicular (CC) distance. For Grade 4-6 the disruption of the AC and CC ligaments and the Deltopectoral Fascia is more severe. For Grade 5 the CC distance is >100% of normal. (2) 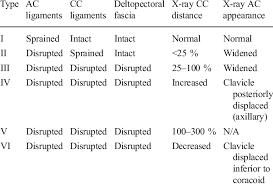 Grade 1-3 Injuries can be managed conservatively with a Broad Arm Sling, Analgesia, an Advice Sheet and discharge. The orthopaedic referral chart (Accessed Oct 2020) states between 0830-2200 Grade 4-6 Injuries should be discussed with the Orthopaedic team on call and between 2200-0830 discussion is not indicated but a fracture clinic triage should be completed. Please ensure Senior ED discussion for all Grade 4-6 Injuries and especially if there is any suspicion of Major Mechanism, Open Injury or Neurovascular Compromise. Ref1. https://faculty.washington.edu/jeff8rob/trauma-radiology-reference-resource/9-upper-extremity/rockwood-classification-of-acromioclavicular-joint-separation/ Ref2. https://www.researchgate.net/figure/Rockwood-classification-of-acromioclavicular-injuries_tbl1_272096166 Steve Fordham Oct 2020 Syncope is a very common presentation to the ED. The ECG is a vital investigation in the context of a transient loss of consciousness / syncope as it can identify the cause, including rare conditions that can lead to sudden cardiac death. The pneumonic WOBBLER can be used as a useful way of asessing the ECG in this context with consideration for these rare causes. W - Wolff-Parkinson-White syndrome – A short PR interval and delta wave: 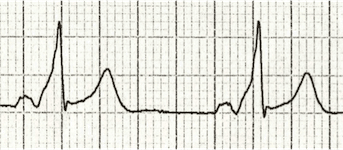 O - Obstructed AV pathway – look for 2nd or 3rd degree block: 2nd degree block: Mobitz type 1 - PR prolongs then QRS not present: 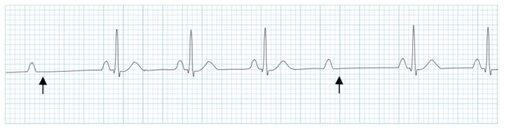 Mobitz 2 - PR Is constant but QRS randomly not present: 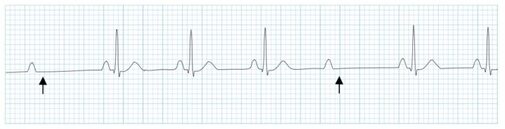 3rd Degree block - complete dissociation between P waves and QRS complexes: 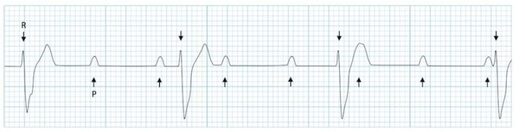 B - Bifascicular block - The combination of axis deviation and right bundle branch block: Bifasicular block has a low risk of deteriorating into complete heart block (~ 1% per year) but trifasicular block (Axis deviation, RBBB and prolonged PR) has a greater risk. B - Brugada - Coved ST elevation (shark fin) followed by a negative T wave in V1-V3 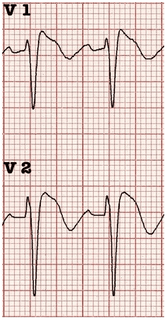 L – Left ventricular hypertrophy - Consider Aortic stenosis and Hypertrophic Obstructive cardiomyopathy (HOCM), these can present with exertional syncope.  LVH diagnostic criteria - S wave in V2 + R wave in V5 > 35 mm E – Epsilon wave - A feature of Arrythmogenic right ventricular dysplasia (ARVD). This is another rare cause of sudden cardiac arrest. The epsilon wave looks a bit like the J wave of hypothermia and may be associated with T wave inversion in V1-V3: 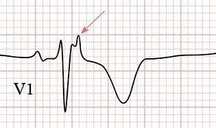 R - Repolarisation abnormality, such as long or Short QT syndrome.
A prolonged QT is > 440ms in men or > 460ms in women. A QT >500ms is associated with increased risk of Torsades de pointes. A QT of <350ms is abnormally short. So thats it, next time you see a patient with a transient loss of consiousness make sure thier ECG is not a WOBBLER. Dr Martin Dore The 3 P's of an uncomplicated faint
Transient loss of consciousness (TLoC) is common but can be a daunting presentation in ED. NICE recommends a simple faint if there are no red flags for cardiac syncope and the 3 P's are present: Posture - prolonged standing Prodrome - sweating or feeling warm/hot before transient loss of conciousness, pallor Provoking factors - pain, medical procedure RED FLAGS
|
This will be an archive of learning blogs and lunchtime learnings bites!
Archives
February 2023
Categories
All
|
 RSS Feed
RSS Feed